A few weeks ago, we had a client walk in complaining of the following issues
- Stiffness in the thigh, groin, or hip
- Deep aching in the groin or butt and hamstring
- Sharp pain in the groin or buttock when the thigh is moved close to the body beyond 90°
- Sharp pain in the groin or buttock when the thigh is moved across the body toward the opposite shoulder
- Pain in the hamstrings with sitting for long periods
- Difficulty with weightbearing on the affected leg
- Hip pain at rest and/or with activity
- Hip pain during and/or after sexual activity
- Pain during or after sports
- Low back pain and/or sacroiliac joint pain (in addition to the other symptoms here)
- Knee pain
- Pain that comes and goes
- Pinchy pain in the front of the hip during deep squats
She had been to the Ortho and a PT, who both (mis) diagnosed her with Hamstring Tendinopathy. She got the Double C treatment (Cortisone and Clam Shells) and after 3 months of that the pain was WORSE than when she started.
After a 2-minute eval, we realized that she, like many other female athletes, had a Femoral Acetabular Impingement (and most likely a labral tear).
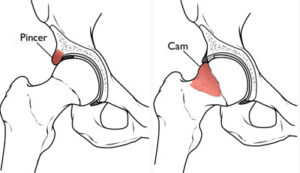
Impingement is the word used to describe a painful contact between two surfaces, which often causes pain.
So we sent her to Dr. Webb at Emory, who did some imaging to rule out the presence of bone spurs or loose bodies. This non-bony impingement is called functional impingement, which is fantastic news!
Because when there is a functional hip impingement (even if there is a labral tear), the data is precise that the treatment and rehab we do are more effective than surgery.
We see this so often that I wanted to share our process, so if you are suffering from a functional hip impingement, you can know that you have hope!

First: Education
A 2012 study actually found that 69% of asymptomatic individuals had hip labrum tears and FAI’s! That means a few thousand people on this email are probably walking around with this issue and do not know it.
Second: We Get Rid Of The Painful Triggers
When an functional impingement is present in the the first thing we have to do is modify al the things that piss of that hip tissue. That means we give you a deep dive plan for changing your sport/workout so you can keep doing things without training.
Third: Put The Damn FIRE Out
Using our unique blend of manual joint mobilizations, dry needling, ART, shockwave, and class IV medical laser, we naturally and without drugs get rid of that pain.
Fourth: Stopping Stretching The Psoas and Start Strengthening It!
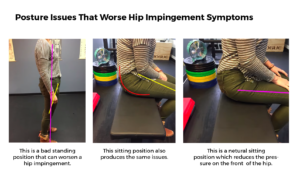
We can get REAL nerdy on this, but we’ll save that for its article. In short, most people that have a hip impingement tend to stand with their butt stuck out and sit with their butt tucked (see images below), which lock the femur into extension which puts a ton of pressure on the front of the hip.
The tendency is to want to stretch the hip, specifically the hip flexors. However, stretching the hip flexors can exacerbate the situation if the hip is chronically in extension, as described above. The misconception is that tightness is due to a muscle being tight and strong. The reality is that the body is either neurologically reacting to stress, or the muscle may be in spasm. Or it may also be your muscle trying to work because it is weak. By stretching it, you are encouraging the problem position of extension, which might irritate an already cranky muscle.
So at ASR, we don’t stretch the psoas of someone with a hip impingement, instead we strengthen it (Kalisvaart & Safran).
Fifth: We Find The Right Biomechanics For You
Everyone’s anatomy is different. Once we have you pain-free and moving strong, we will find the correct form (for you) for squatting, running, hinging, sitting, etc. We will teach you how to self-identify and correct errors and then release you back to the wild where you can be a statistic of someone who operates at 100%, despite their functional hip impingement, rather than someone who had surgery on it and still has the same issues.